Enlarged Vestibular Aqueduct Syndrome
Enlarged vestibular aqueduct syndrome, or EVA, is a rare condition affecting the inner ear. Children with EVA often experience hearing loss that they are either born with, or which can develop and progress throughout childhood and into adulthood.
Because EVA is so rare – affecting fewer than 200,000 people nationally – there is relatively little scientific research compared to other diseases. Many unanswered questions remain about the causes, diagnosis and treatment of patients with EVA.
The team at University Hospitals Rainbow Babies & Children’s are experts in EVA and hearing loss. Their research is providing insight into this rare condition to improve outcomes for patients around the world.
Make an Appointment Today
Call 216-UH4-KIDS or schedule online with one of our pediatric ENT providers.
EVA Patient Registry
Enroll in the EVA patient registry.
Hearing Loss Risk Calculator
Estimate the probability of hearing loss progression.
Donate to Research
Learn about ways to support our ongoing research efforts.
What Is Enlarged Vestibular Aqueduct Syndrome?
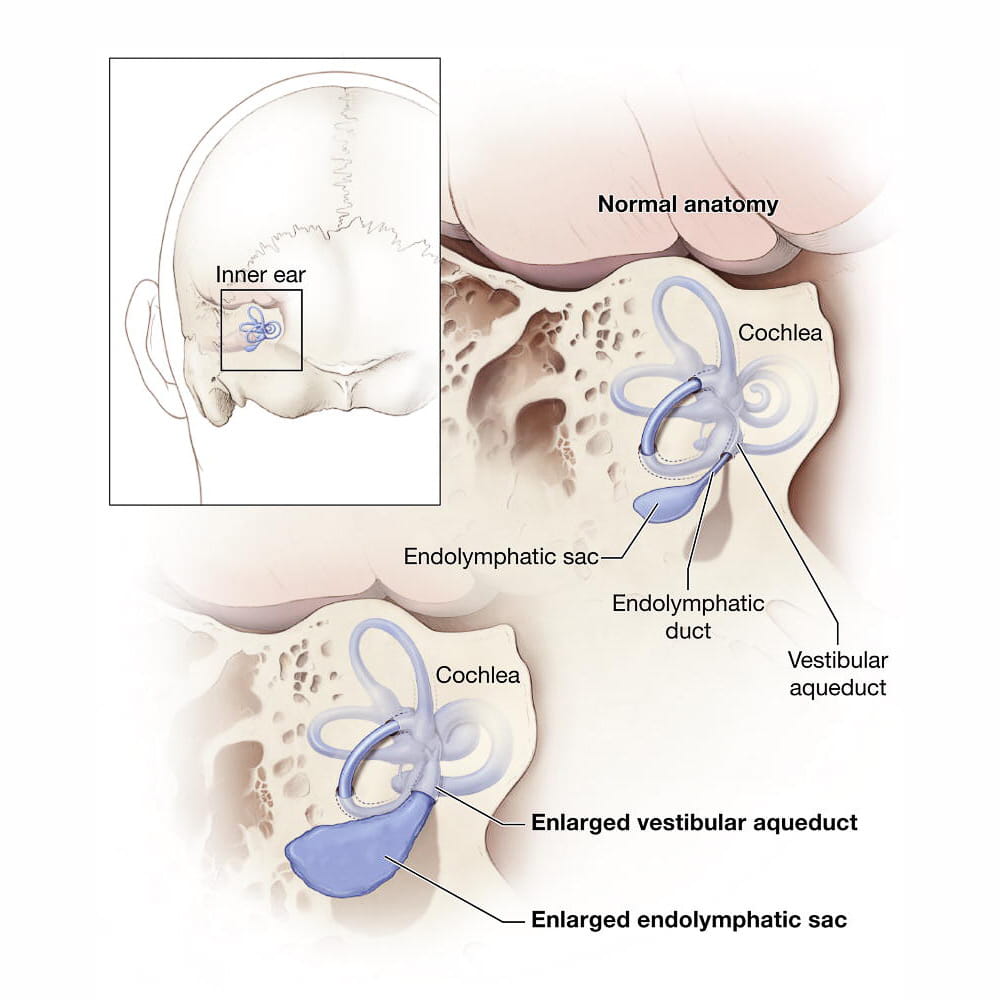
The vestibular aqueduct is a narrow tube filled with fluid in the inner ear. It is located in the temporal bone of the skull behind the ear and connects the inner ear to a balloon-shaped structure called the endolymphatic sac. The inner ear consists of the cochlea and vestibular apparatus, which control hearing and balance respectively. These structures send signals to the brain to help process sound and support the body’s sense of balance. Abnormalities in these structures may contribute to hearing loss, balance problems or both.
The vestibular aqueduct is considered enlarged if it larger than 1 millimeter, about the size of the head of a pin. Children with EVA may also have an enlarged endolymphatic duct (which runs through the vestibular aqueduct) and endolymphatic sac.
Causes of EVA
The exact cause of EVA is unknown but there are likely a number of contributing factors. These include a gene mutation known as SLC26A4 that can cause EVA, Pendred syndrome and hearing loss. Other genetic and environmental factors may be at play in EVA.
EVA and Hearing Loss
Most children with EVA develop some degree of hearing loss, although the timing and severity varies for each child. About 5–15 percent of children who are diagnosed with sensorineural hearing loss – or hearing loss caused by damage to the inner ear – have EVA. However, the hearing loss may be caused by an underlying anatomical defect and not the EVA itself. The identification of EVA can be an important clue to understand all causes of the hearing loss.
About 25 percent of people with EVA have Pendred syndrome, which is characterized by hearing loss and thyroid disease. The hearing loss associated with Pendred syndrome is often progressive, resulting in more severe hearing loss or deafness.
Children with EVA-related hearing loss may also have problems with their balance. Fortunately, these balance difficulties are typically brief and mild. If balance issues are more problematic, vestibular (balance) testing with vestibular rehabilitation may be required.
It is not entirely understood how abnormalities in the inner ear contribute to sensorineural hearing loss. Experts believe that the fluids in the endolymphatic duct and sac must remain in careful balance, because even minor changes may lead to hearing loss.
Diagnosing EVA

EVA is usually diagnosed while trying to determine the source of a child’s hearing loss. When hearing loss is suspected, your child’s physician will conduct an age-appropriate hearing (audiometry) test to determine the presence and severity of the hearing loss. Additionally, they may conduct auditory brainstem response testing (ABR), which uses electrodes attached to the skin to record brainwave activity in response to sound.
Once sensorineural hearing loss has been confirmed, imaging scans such as magnetic resonance imaging (MRI) and computed tomography (CT) may be recommended to evaluate the inner ear structure. Although most imaging results are normal, when there is an anatomic abnormality, EVA is the most common.
Early Diagnosis Reduces EVA’s Impact
Identifying hearing loss as early as possible is the best way to reduce EVA’s impact. The earlier hearing loss is identified in children, the sooner they can develop skills that will help them learn and communicate with others. Children with permanent and progressive hearing loss, which often is linked with EVA, will benefit from learning other forms of communication, such as sign language or cued speech, or using assistive devices, such as a hearing aids or cochlear implants.
EVA Treatment and Management
There are no routine medical or surgical treatments for EVA. In fact, research has shown that surgical procedures to drain liquid from the endolymphatic duct and sac or to remove them are not only ineffective in treating EVA, they can be harmful and worsen hearing.
There is some anecdotal evidence that a course of steroids may be helpful at restoring some hearing in cases where sensorineural hearing loss is sudden in patients with EVA. However, more research on this topic is needed.
Reducing the Risk of Hearing Loss with EVA
Certain activities are associated with increased hearing loss in children with EVA. These activities should either be avoided or proper precautions should be taken to reduce the risk of injury or trauma. These include:
- Contact sports and activities: Any activity where the participant could sustain a head injury or barotrauma (ear damage caused by pressure differences between the middle ear and the outer ear) could cause further damage and hearing loss. Activities such as contact sports, cycling and skiing should be undertaken with protective headgear or avoided altogether.
- Activities with rapid changes in air pressure: Activities such as scuba diving and hyperbaric oxygen treatments should be carefully avoided because of their risk of sudden worsening of hearing loss.
- Air travel: Pressure changes with air travel have also been reported to cause hearing loss in EVA patients. However, this is rare in commercial aircraft with pressurized cabins, and this risk may be minimized by taking a nasal decongestant before travel, particularly if there is sinus or nasal congestion.
EVA Research Project
Researchers at UH Rainbow Babies & Children’s Hospital are investigating the causes, diagnosis and management of EVA and related hearing loss. Through the creation of a patient registry, our research team is collecting and compiling individual patient data in order to better understand EVA. This includes examining the condition’s different symptoms, hearing loss prognosis, and risk factors for hearing loss progression. Our hope is that through our dedicated research efforts we can contribute new prevention, treatment and rehabilitation options for children with EVA-related hearing loss.