

Making the Case for CT CORONARY CALCIUM SCORING
January 16, 2017
Innovative, no-cost program increases access to vital test
Harrington Heart & Vascular Institute Innovations – Spring 2016, updated January 2017
 David A. Zidar, MD, PHD
David A. Zidar, MD, PHD Robert C Gilkeson, MD
Robert C Gilkeson, MDPreventive cardiologists continue to refine their risk prediction models, striving for the “perfect formula” for predicting a heart attack or other cardiovascular event. Yet many of these specialists acknowledge there is still much to be learned.
“These models aren’t as good as we’d like them to be at identifying high-risk people,” says David Zidar, MD, PhD, Director, Familial Dyslipidemia/LDL Apheresis Clinic, UH Harrington Heart & Vascular Institute; Assistant Professor of Medicine, Case Western Reserve University School of Medicine. “We have risk scores that rely on some of the traditional cardiac risk factors, but they’re not always adequate for us to drill down and focus our efforts on specific populations.”
At UH Harrington Heart & Vascular Institute, preventive cardiologists are addressing this issue by supplementing traditional risk scoring with an aggressive coronary calcium scoring program. Begun in 2007, the program has provided 15,000 coronary calcium tests to date for UH patients.
“The coronary calcium score allows us to reclassify a patient’s risk for heart attack or stroke, more accurately than if they had a ranking based solely on traditional risk factors,” Dr. Zidar says.
To increase access, the test was originally made available on a self-pay basis of $99.
“We decided early on that we weren’t going to let cost be an issue in terms of access to this technology,” says Robert Gilkeson, MD, Director, Cardiovascular Imaging Center, UH Harrington Heart & Vascular Institute; Professor of Radiology, Case Western Reserve University School of Medicine. “As a result, we’ve been able to much more appropriately risk-stratify and prescribe statin therapies for our patients.”
Coronary calcium scoring is available at UH Cleveland Medical Center through the UH Harrington Heart & Vascular Institute, as well as multiple UH community hospitals and ambulatory health centers. The program has grown from about 100 tests per month, systemwide, to about 200. During a June 2015 pilot, the test was offered at no-cost and attracted 800 patients – including a significant number of women.
“We know that women tend to under-report and under-treat symptoms of heart disease,” Dr. Gilkeson says. “When we offered the test at no-cost, the proportion of women went from 40 percent to 60 percent – and we saw severe disease in about 15 percent of them.”
In follow up to the pilot, University Hospitals now offers the CT coronary calcium score test at no-cost across the UH system for all at-risk patients.
| CACS | 10-Year Risk of Nonfatal MI or CHD Death |
Risk Stratification |
|---|---|---|
| 0 | Less than 1% | Lower |
| 1 - 99 | 4% | Lower to moderate |
| 100 - 399 | 13% | Moderate |
| 400 or greater | 24% | High |
For Dr. Zidar, it’s a matter of having another tool in the arsenal.
“Coronary calcium scoring is not right for everyone, and it’s absolutely not right for people who are having symptoms, such as chest pain,” Dr. Zidar adds. “Chest pain requires evaluation with stress testing or fractional flow reserve-CT angiography (FFR-CT).”
UH Harrington Heart & Vascular Institute launched a new program in 2016 – ICE (Inflammatory Cardiovascular disease Elimination) Cardiology – that focuses on the prevention of cardiovascular disease in patients with chronic inflammation. Inflammation drives the initiation and progression of atherosclerosis, and is also linked to plaque rupture and thrombosis that cause heart attack and stroke. Individuals with rheumatologic (systemic lupus erythematosus, rheumatoid arthritis, ankylosing spondylitis, scleroderma), inflammatory bowel (ulcerative colitis, Crohn’s disease), and skin (psoriasis) disease are known to be at increased risk of cardiovascular disease. Risk prediction in these individuals is challenging and may be improved substantially with the use of CAC scoring.
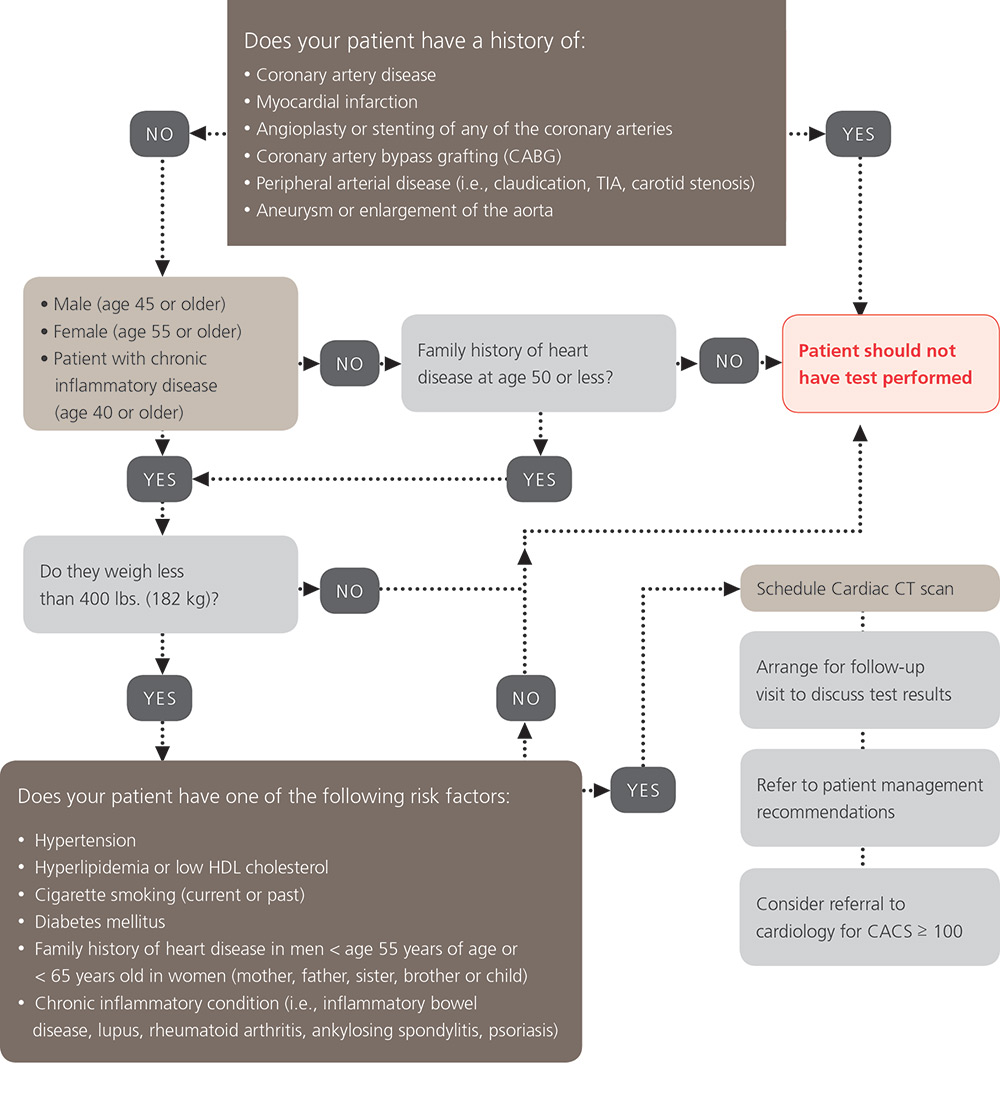
To refer a patient for CT coronary calcium scoring, please call Radiology Central Scheduling at 216-844-1700. For more information, and to download the latest materials related to this program, including an appropriateness algorithm, patient management recommendations and patient information sheets, click here.
Tags: Calcium Scoring