

A Game-Changer for Assessing Cardiac Risk
June 14, 2022
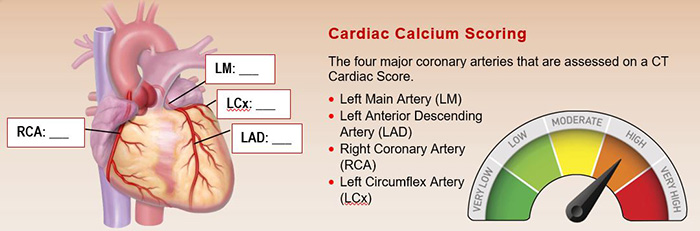
New criteria for no-cost Coronary Artery Calcium Scoring allows the test to be used for a broader population
UH Clinical Update | June 2022
Only at University Hospitals can patients receive a simple test – at no charge – that can reveal such vital information about their risk for a heart attack.
And yet that is exactly what UH has done for more than seven years, helping tens of thousands of Northeast Ohioans learn whether they have coronary artery disease and their risk for a future devastating event like a heart attack and/or stroke.
“This way of making prevention ‘no cost’ to the patient is a game-changer,” says Sanjay Rajagopalan, MD, Chief of Cardiovascular Medicine and Chief Academic and Scientific Officer for University Hospitals Harrington Heart & Vascular Institute and the Herman K. Hellerstein, MD, Professor of Cardiovascular Research. “This no-cost approach is not available in any other part of the world except in this corner of Northeast Ohio. Nobody subsidizes prevention but this is exactly what is needed to change the practice of medicine.”
‘This program is a great example of the active collaboration between cardiology and radiology to optimize the delivery of care,” says Chip Gilkeson, MD, Division Chief of Cardiothoracic Imaging of at UH Cleveland Medical Center.
UH Harrington Heart & Vascular Institute now recommends Coronary Artery Calcium Scoring (CACS) for all women and men 45 and older with certain risk factors. Click here for the full list of risk-enhancing indications for coronary calcium scoring. For certain individuals with known cardiovascular risk, including those with conditions such as rheumatoid arthritis or kidney failure, or who have experienced premature menopause, the test may be done before age 45.
UH Harrington Heart & Vascular Institute partnered with UH Radiology to ensure access for this noninvasive CT scan of the heart, which requires just a 30-minute appointment with only five to 10 minutes on the scanner and no contrast used. While that test is a cost for the system, it’s of immeasurable benefit for patients and the health system in caring for patients’ long-term health. Radiology performs more than 14,000 CACS tests each year, at every radiology site in the UH system.
The current success of the CACS program has been more than 15 years in the making. In 2006, former UH preventive cardiologist Carl Orringer, MD, contacted Dr. Gilkeson to tout the advantages of CACS in detecting cardiac risk. But at the time, the test cost $500 and was not covered by insurance. However, the UH team was not deterred. Ultimately, Dan Simon, MD, then President of UH Harrington Heart & Vascular Institute, and colleagues successfully advocated for a novel $99 self-pay CACS program for Northeast Ohio patients.
“Even then, it was a significant departure because of the low cost –-significantly less than a conventional Cardiac or Chest CT,” Dr Gilkeson says. Dr. Gilkeson then worked with his radiology and cardiovascular colleagues to provide the clinical expertise necessary and the training and referrals to make it happen – not an insignificant undertaking.
“It is a technically demanding test to perform,” he says. “While it is a fast exam – five to 10 seconds -- the acquisition of the CT scan must be synchronized to the patient’s EKG.”
Low-cost CACS continued for several years, attracting 25 to 30 patients a month at first. But as it became clear that the downstream diagnostic benefits of CACS in detecting cardiac risk in asymptomatic patients were so significant, UH made the decision in 2018 to offer CACS at no cost to patients.
The response from the public was overwhelming, increasing demand for the test by a factor of 10, from about 80 a month to 800. The demographics of patients choosing to have the test changed, too, with more women and more patients with serious disease taking advantage of it
In the years since, the UH team lead by Dr. Rajagopalan has published widely on its successes with no-cost CACS. This began with the first publication of the program that brought attention to what UH is doing in Northeast Ohio in the prestigious journal Journal of the American College of Cardiology. This widely cited paper detailed the impact of the no-cost program, particularly its impact on increasing the percentage of African-American and women who benefited from the no-cost program.
Dr. Rajagopalan and colleagues followed up with another impactful paper on the benefit of the program in the American Journal of Cardiology, which found that provision of no-cost CACS among 50,000 patients allowed physicians to reclassify the 10-year atherosclerosis risk for approximately one in five patients and resulted in improved treatment approaches such as increased utilization of statin therapies. UH Harrington Heart & Vascular Institute cardiologist Sadeer Al-Kindi, MD, was first author on the paper, which also included Nour Tashtish, MD, Imran Rashid, MD, Amit Gupta, MD, Kianoush Ansari Gilani, MD, Peter Pronovost, MD, PhD, as well as Dr. Simon and Dr. Gilkeson. Following on that, Dr. Gupta and UH radiology colleagues recently published a study on CACS in the journal Radiographics, the most widely read imaging journal in the world. Co-authors on this recent paper include UH physicians Kaustav Bera, MD, Elias Kikano, MD, Jonathan D. Pierce, MD, and Maharshi Rajdev, MD, as well as UH radiology supervisor Leslie M. Ciancibello, RT, medical student Jonathan Gan, and Dr. Rajagopalan and Dr. Gilkeson.
A no-cost approach to CACS is a perfect example of UH’s commitment to population health, utilizing technology to impact an entire community and population health on a massive scale.
“The true benefit of this program is that we’ve taken the cost barrier away and have improved patient outcomes. Importantly, the test also may help alert other concomitant conditions within the imaging field of view,” Dr. Gilkeson says.
“In many ways, we at UH are trend setters,” adds Dr. Rajagopalan. “CACS provides a much better barometer of your cardiac health than any of these isolated numbers like your cholesterol, blood pressure scores or markers such as CRP or high-sensitivity troponin values. It provides preemptive identification of disease that is very specific, actionable at the physician and patient level.
“In medicine in general and in cardiology in particular, we get excited about technology, but technology solutions for precision care are often high cost and do not translate to better outcomes for our patients. CACS at no cost is a high-technology scalable approach to precision health that UH has invested in to bring value to patients.”
UH Harrington Heart & Vascular Institute is finalizing a newly designed report that will provide each patient who undergoes CACS with details of their cardiac risk in full color with pictures. Written at an eighth-grade reading level, the report explains in simple terms a patient’s current and 10-year cardiac risk of heart attack and needed follow-up. Patients can better understand if they need blood pressure or statin medications, or more invasive follow-up such as cardiac catheterization.
“Prevention cannot be monetized,” says Dr. Rajagopalan. “How can you put a value on the life that you have saved? Prevention is truly impactful, saving millions of lives.”